
If you are here because how much does ivf cost feels like a simple question with a complicated answer, I want you to know you are not behind, and you are not “too sensitive” for caring about the money side of medicine. Cost is part of care. And when endometriosis is involved, the plan can quietly expand, with more testing, more time, and more steps. So, in this guide, I will walk with you through what endometriosis is, how it can affect fertility and IVF outcomes, and which parts of a treatment plan tend to change the budget most.
As a reconstructive urologist who works with men and couples around sexual health, fertility, and confidence, I have seen how uncertainty can strain a relationship. So, we are going to make this clearer. Step by step. And with respect for both your goals and your limits.
Introduction: Why this topic matters (and why it often gets missed)
Endometriosis is common. Yet it often hides in plain sight. Many people live with symptoms for years before a clear diagnosis. That delay can matter, especially when you are trying to build a family.
What makes this emotionally hard is the “double burden.” First, pain and fatigue can wear someone down. Then, infertility can arrive as a shock, even when periods seemed “normal enough.” Meanwhile, the male partner may feel helpless, guilty, or pressured to fix something he cannot control. Have you noticed how quickly intimacy can turn into a calendar and a performance test?
In the fertility webinar this outline is based on, the expert lays out a practical path: understand the condition, understand how it affects fertility and IVF, and then choose treatment options that match the person’s age, symptoms, and goals.
This matters now because more couples are asking for transparency. They want a plan that respects time, mental health, and finances. That is reasonable. And it is achievable.
What endometriosis is (plain-English explanation)
Endometriosis is when tissue similar to the uterine lining shows up outside the uterus. It can appear on the tubes, ovaries, the tissues around the uterus, and even on the intestines or bladder. In some cases, it can show up in distant places such as the diaphragm or in surgical scars.
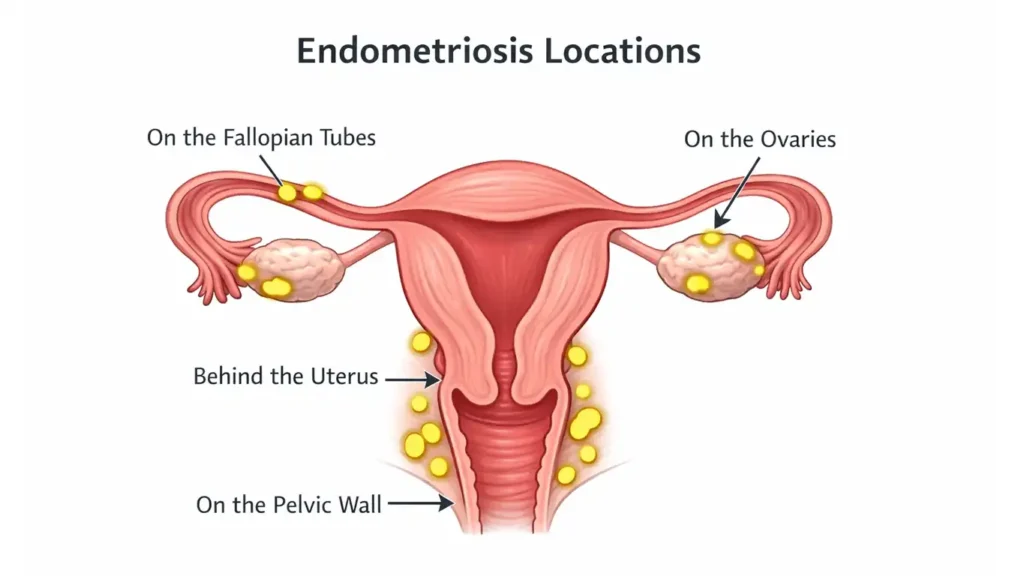
Here is the key idea. These areas can bleed in tiny amounts during a cycle. But unlike a period, that blood has nowhere easy to go. As a result, the body reacts with inflammation. Over time, that inflammation can lead to fibrosis, which is scar tissue.
Think of it like a small, repeating injury. Even when each episode is “minor,” the cumulative effect can be major. That is why someone can have real symptoms even if imaging looks “not that bad.”
If you are a partner reading this, here is a useful mindset: endometriosis is not “in someone’s head.” It is a real, physical process. And acknowledging that reality can lower tension at home.
How common it is (and why diagnosis is delayed)
Endometriosis affects about 1 in 10 women, and estimates suggest it impacts roughly 200 million women worldwide. It is often identified around ages 30 to 40, but it can start much earlier.
So why the delay? Because symptoms vary, and they can overlap with many other conditions. Some people are told their pain is “just cramps.” Others are treated for digestive issues. Some are sent for back workups. And many are placed on hormonal birth control, which can reduce symptoms and make the condition harder to recognize.
Diagnosis delays are often measured in years, not months. That is frustrating. Also, it can change fertility planning. If someone waits until the pain is severe or until infertility is the first clear signal, the timeline can suddenly feel tight.
If you feel like the story of symptoms has been long and confusing, that is not a personal failure. It is a known pattern of this disease.
Symptoms: the “chameleon, iceberg, time bomb” reality
Endometriosis can look different from person to person. Some people have severe pain. Others have mild pain but significant fertility issues. And some have symptoms that come and go.
Common symptom clusters include:
- Tiredness or low energy
- Abdominal pain
- Painful periods
- Pelvic pain
- Back pain
- Bloating
- Pain with sex
- Pain with bowel movements
- Pain with urination
The webinar used three helpful metaphors:
Chameleon
- Symptoms can change over time.
- What was once “just cramps” can evolve into pelvic pain, bowel pain, or deep fatigue.
Iceberg
- What you see on a scan may not reflect the full depth of disease.
- Some disease can be hidden under the surface.
Time bomb
- Sometimes symptoms stay quiet until infertility becomes the first major signal.
Pro Tip 🧠: Keep a simple symptom log for 2 to 3 cycles. Note pain, bowel or bladder symptoms, fatigue, and how it affects sex. This helps you tell a clear story in the clinic.
And here is a question worth asking: have you or your partner started avoiding intimacy because you fear pain, conflict, or disappointment? Naming that early can protect the relationship later.
Endometriosis and infertility: how the condition can reduce fertility
Endometriosis is linked to infertility in a significant portion of women, and it shows up more often in infertility populations than in the general public.
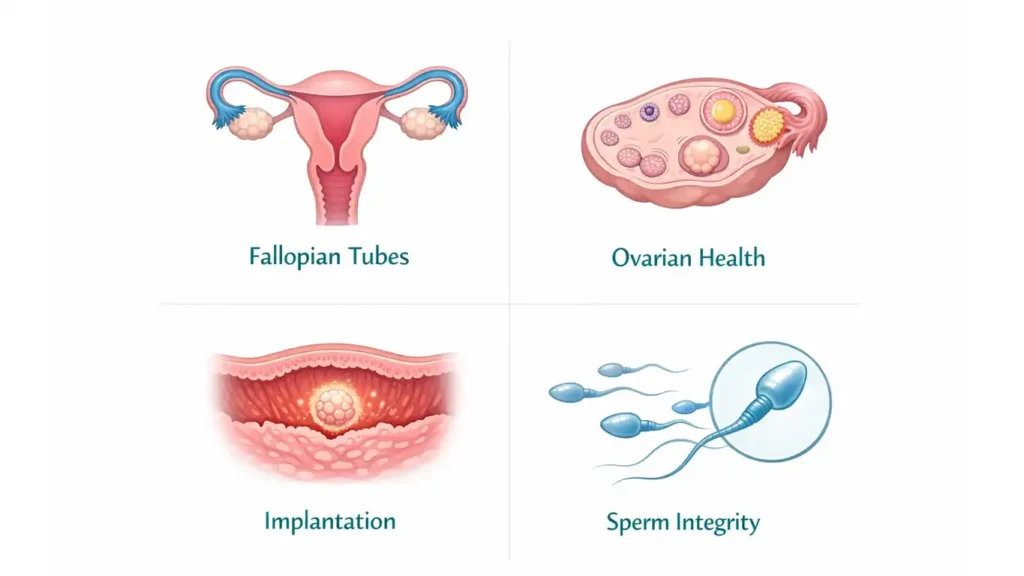
There are several pathways:
Fallopian tubes
- Inflammation and scar tissue can affect tube function.
- Adhesions can distort anatomy.
- In some cases, fluid issues can interfere with natural conception.
Ovaries and eggs
- The condition can affect follicle development and growth.
- Oxidative stress is discussed as a possible mechanism.
Uterus and implantation environment
- The lining environment may be altered, which can affect implantation readiness.
Sperm effects
- The webinar also noted potential impacts on sperm integrity and function.
- This is one reason I encourage couples not to ignore the male side of the workup, even when endometriosis is present.
So, endometriosis is not one single “problem.” It can be a network of effects. That is why the best plans tend to be personalized.
What endometriosis can mean for IVF success
The webinar highlighted several IVF impacts associated with endometriosis:
- Lower implantation rates
- Fewer eggs retrieved
- Higher ectopic pregnancy risk
That does not mean IVF will not work. It means the inputs and expectations may change. For example, if fewer eggs are retrieved, a couple may need to think about the possibility of multiple IVF cycles. And when people feel anxious, they sometimes push for transferring more embryos to “over-correct.” However, that can increase the risk of multiples, which carries its own medical and financial burdens.
This is where the concept of IVF success rate vs cost becomes real. A choice that seems cheaper in the short term can create expensive complications later.
Also, age matters. IVF outcomes tend to decline with age, and endometriosis can add another layer. That is not meant to scare you. It is meant to help you plan.
Ask yourself: are you looking for certainty, or are you looking for the next best step that protects your future options?
Pregnancy outcomes after conception: what to watch for
Once pregnancy happens, the webinar noted specific risks that may be higher with endometriosis:
- Higher chance of placenta previa
- Higher rates of bleeding
At the same time, the expert also offered reassurance. They did not describe major differences in live birth rates, low birth weight, or neonatal complications in the way many people fear.
So what does this mean for you? It means prenatal care may include more attention to placenta location and bleeding symptoms. And it means you should not assume that endometriosis automatically equals a “bad pregnancy.”
If you are the male partner, here is a practical role you can play: be the calm record keeper. Go to visits when you can. Ask questions. Help reduce the mental load at home. This is not just medical. It is relational.
Treatment goals when fertility is part of the plan
When fertility is on the table, the goal is balance. You want symptom relief. You also want to protect reproductive potential. Those goals can align, but sometimes they compete.
The webinar used a useful phrase: a “conservatively radical” approach. In other words, treat what needs treating, but avoid unnecessary radical steps that could harm ovarian reserve or future options.
Decision factors include:
- Age and overall health
- How extensive the disease is
- Other infertility factors in the couple
- Pain severity and quality of life
- The patient’s wishes and timeline
In my world of men’s sexual and reproductive health, I have learned something that applies here too: when patients feel rushed or unheard, outcomes suffer. So, shared decision-making is not a “nice extra.” It is central.
Pro Tip 🧾: Ask your clinic for a written, itemized plan before you start. It lowers stress and reduces surprise bills.
And here is a gentle question: what would “success” look like for you, beyond a positive test? More peace? Less pain? A plan you can sustain?
Why multidisciplinary care is a big deal (not optional, per the speaker)
Endometriosis is not a one-specialty condition. The webinar emphasized multidisciplinary care.
That team can include:
- Specialist gynecologist
- Fertility specialist
- Minimally invasive or robotic surgeon
- Imaging specialists (ultrasound, MRI)
- Pain management
- Nursing support
- Psychologist or counselor
- Colorectal or urology surgeons when needed
This matters because the disease can involve multiple organs and multiple life domains. Pain affects sleep. Sleep affects mood. Mood affects sex. Sex affects relationship stability. And relationship strain can make treatment feel heavier than it already is.
If you are a couple, I strongly suggest you treat the team like a team. You do not have to carry the whole plan alone. Support groups can also help, including fertility support and advocacy resources and endometriosis education and awareness resources.
Treatment options discussed in the webinar (organized for readers)
Medical options (symptom control and fertility context)
Medical options can include hormonal manipulation, suppression, or down-regulation, as well as contraceptives. The webinar also mentioned anti-inflammatory and antioxidant agents as add-ons, but with uncertain outcomes.
A key idea from the Q and A: endometriosis lesions can bleed internally, and hormonal treatment may aim to stop periods and reduce that cycle-driven inflammation. In some cases, response to hormonal suppression can also support the clinical suspicion when diagnosis is unclear.
Medical therapy is not a moral choice. It is a tool. For some people, it buys time. For others, it reduces pain enough to function while planning the next step.
If you are the partner, this is where empathy matters. Hormonal shifts can affect mood and libido. So, the question is not “why are you different?” The question is “how do we support you through this season?”
Fertility-focused options for couples asking how much does ivf cost
Fertility-focused options can include:
- Pre-IVF testing and counseling
- Individualized IVF and ICSI approaches
- Egg donation in cases of advanced age, repeated failures, or very low ovarian reserve
- Surrogacy in certain uterine factors discussed by the speaker
Below is a practical IVF cost breakdown table you can use to ask better questions. It is not a price list. Instead, it shows the line items that commonly shape IVF out-of-pocket cost, especially when endometriosis changes the plan.
| Line item you may see | What it often covers | Why it may change with endometriosis |
|---|---|---|
| IVF consultation cost | Initial physician visit, plan building | More time spent on history, symptoms, imaging review |
| IVF monitoring cost | Ultrasounds, bloodwork, follow-up visits | Closer monitoring may be needed based on risk and response |
| IVF cost per cycle | Core cycle services (clinic dependent) | May take more than one attempt, so multiple IVF cycles cost becomes relevant |
| average IVF cost in the US | Benchmark term people search | Real totals vary by region, lab, and coverage |
| IVF clinic pricing comparison | Comparing clinics and package structure | Packages differ on what is included vs extra |
| IVF cost with insurance | Coverage, prior auth, exclusions | Endometriosis care may trigger additional criteria or denials |
| IVF financing options | Payment plans, loans, clinic partners | Helpful when timelines are tight and costs stack |
| IVF medication cost | Stimulation meds, triggers, support meds | Protocols may differ, and suppression can add time and meds |
| egg retrieval cost | Procedure and anesthesia | Ovarian factors can affect planning |
| embryo transfer cost | Transfer procedure, monitoring | Strategy may shift based on outcomes and risk |
| frozen embryo transfer cost | Frozen transfer cycle | Used when timing or uterine prep needs optimization |
| embryo freezing storage fees | Cryopreservation and annual storage | More common when banking embryos over time |
| ICSI cost | Fertilization technique | Often used when sperm factors are present or suspected |
| PGT testing cost | Embryo genetic testing | Considered in some scenarios, depends on goals |
| PGT-A cost | Aneuploidy screening | Sometimes considered to reduce uncertainty |
| IVF add-ons cost | Extra lab or procedural add-ons | Important to ask what evidence supports each add-on |
| endometriosis IVF cost | Endometriosis-related planning costs | Imaging, prolonged protocols, or surgery can add steps |
| endometriosis surgery before IVF cost | Surgical evaluation and excision | May be recommended in specific cases |
| laparoscopy endometriosis cost IVF | Laparoscopic surgery path | The webinar noted pregnancy rate improvements after laparoscopic management in some settings |
| GnRH suppression before IVF cost | Down-regulation protocol | May be used to reduce inflammation before transfer |
| endometrioma IVF cost considerations | Ovarian cyst management planning | The webinar cautioned against draining endometriomas before IVF |
| ectopic pregnancy risk endometriosis IVF (cost planning keyword intent) | Risk-driven monitoring and care | Higher risk can mean more monitoring and contingency planning |
If your clinic offers a package, ask: what is included, and what is billed separately? Also ask: if this cycle does not work, what costs repeat, and what costs do not?
Surgical options (minimally invasive, laparoscopy, robotic)
The webinar described laparoscopy as a long-time gold standard. It also discussed robotic surgery as a state-of-the-art approach for severe or deep infiltrating disease, especially in repeat surgery cases. Benefits mentioned included precision, 3D visualization, and safer excision with better protection of nerves and vessels.
A critical point was the “iceberg” issue. Disease can be deeper than what is seen on the surface. Even surgery can miss lesions if they are not recognized.
Surgery can help in some fertility contexts. Yet it must be individualized, because ovarian tissue matters.
Emerging or experimental options (briefly mentioned)
The webinar briefly referenced emerging areas such as molecular targets, gene expression, prostaglandin inhibitors, and stem cell related work. These are not standard care for most patients right now. So, I advise you to treat them as “watch this space,” not “bet the house.”
If you see flashy marketing online, pause and ask: what is the evidence, what are the risks, and what does it cost?
Patient practicalities: what to do with this information (how much does ivf cost)
Start by getting clear on your situation:
- What symptoms are present, and how do they affect daily life and sex?
- What testing has already been done?
- Are there other infertility factors in the couple?
- What is your timeline, emotionally and financially?
Next, plan your clinic conversation. Bring your symptom log. Bring prior records. Ask for a written plan and a clear explanation of the “why” behind each step.
Also, protect the relationship. Infertility stress can create distance, even in strong couples. So schedule a weekly check-in that is not about calendars or labs. Ask each other: what do you need this week to feel supported?
Pro Tip 🤝: Go to at least one key appointment together. Two sets of ears reduce mistakes, and it also reduces the feeling that one partner is carrying everything.
If you need additional education, you can review CDC information on assisted reproductive technology as a general reference point for how IVF is tracked and reported.
Webinar Q&A: reader questions you can mirror as FAQs in the article
Does endometriosis make IVF results worse as I get older?
The webinar answer was yes. Age affects IVF outcomes, and endometriosis can add a negative effect.
So, the practical takeaway is timing. If you are deciding between “wait and see” and “make a plan,” a plan usually wins. That plan can include fertility preservation in younger patients, or a clear attempt strategy when time is limited.
A question to ask your clinic is: what is our strategy if we get fewer eggs than expected? That single question can prevent confusion later.
Oxidative stress was mentioned. Should I take supplements like ubiquinol?
The webinar described oxidative stress as a proposed mechanism, but it did not present a definitive supplement protocol. The tone was cautious. Some supplements may not be harmful, but they are not a guaranteed fix.
My advice is simple. Do not use supplements as a substitute for a medical plan. And do not let expensive “stacks” drain your budget without a clear purpose.
Ask: which supplements do you recommend, why, and for how long?
Can hormonal birth control mask endometriosis symptoms?
The webinar response was yes. Birth control can reduce symptoms and make the condition less obvious.
This is why the chameleon and time bomb metaphors matter. Less pain does not always mean less disease. Sometimes it means symptoms are quieter.
If you stopped birth control and symptoms surged, that is a clinical clue worth discussing.
Is endometriosis fed by estrogen only, or progesterone too?
In the Q and A, the speaker explained the core idea in simple terms: lesions can respond to the hormones that drive cycles. So, treatments that stop periods can reduce the internal bleeding and inflammation that worsen symptoms.
If you feel confused by hormone talk online, you are not alone. The key is not “one hormone is evil.” The key is how the cycle signals affect the lesions in the body.
Do you drain endometriomas before IVF?
The webinar speaker said no. Reasons included:
- A cyst may not be an endometrioma.
- The contents may be clotted and hard to drain.
- There is infection risk with needle puncture.
- Inflammation and spillage are concerns, and embryos do not thrive in inflamed environments.
- There is also a caution not to assume. Cancer must be considered and ruled out when appropriate.
So, if someone tells you “we can just drain it,” ask what the risks are and what alternative strategies exist.
I am 41 with severe endometriosis, low AMH, and failed transfers. What now?
The webinar guidance was practical. Continue IVF as long as eggs and embryos can still be produced, while recognizing that protocols vary. Options discussed included down-regulation length, anti-inflammatory approaches such as steroids, and decisions around fresh vs frozen transfer.
If repeated transfers fail, the speaker mentioned considering egg donation.
I know this is emotionally heavy. So here is a question that often helps: do you want to optimize for a genetic connection, or do you want to optimize for becoming a parent, as soon and as safely as possible? There is no wrong answer. There is only your answer.
Can endometriosis be prevented?
The webinar answer was no, not currently. The focus is awareness, earlier detection, and better education across specialties.
This is why taking symptoms seriously matters. It is also why advocacy matters, especially in young patients who are told pain is “normal.”
If endometriosis is only on one ovary, is the other safe?
The webinar suggested it can be localized in some cases, and it emphasized careful imaging, possible laparoscopy, and follow-up.
So, ask your clinician: what is our monitoring plan, and what would trigger a change in strategy? Clarity reduces anxiety.
Autoimmune issues and recurrent implantation failure. Should I do immune treatment or suppression?
In the Q and A, the speaker supported avoiding risky excision near key nerves if symptoms were controlled. They also discussed considering longer GnRH analogue suppression to reduce inflammation, while noting the evidence is not always clear, and they mentioned steroids for anti-inflammatory or immunosuppressive effect.
This is a “personalized medicine” moment. The right plan depends on your history and risk profile.
Is endometriosis linked with obesity?
The webinar speaker said they were not aware of an association and did not answer beyond that.
When an expert says “I don’t know,” I respect it. Medicine needs more of that honesty.
Conclusion: Take-home messages and patient call-to-action
Endometriosis is common. It can affect quality of life, fertility, and IVF outcomes. However, it is not a dead end. The most important shift is moving from vague worry to a concrete plan.
Here are the take-home points from the webinar lens:
- The condition can be hard to diagnose, and delays are common.
- It can reduce implantation rates, reduce eggs retrieved, and raise ectopic risk.
- Pregnancy risks like placenta previa and bleeding may be higher, yet outcomes can still be reassuring in key areas.
- Treatment is challenging, so specialized care and multidisciplinary teams matter.
- Options include medical therapy, fertility-focused approaches, and surgery, including minimally invasive and robotic methods in selected cases.
- “Conservatively radical” means treat what matters, protect what matters, and keep the person’s goals central.
If you do one thing after reading this, do this: write down your top three concerns, your timeline, and your budget boundaries. Then bring that to your care team. You deserve a plan that fits your life, not a plan that breaks it.

 By
By
 By
By




 By
By
 By
By


 By
By




