
Introduction: More Than Just Occasional Heartburn
Throughout my career caring for patients with complex chronic conditions, I’ve witnessed how untreated GERD creates cascading health complications that extend far beyond digestive discomfort. Many men I treat for genitourinary issues also struggle with severe reflux that disrupts their sleep, compounds their anxiety, and erodes their overall quality of life. The silent progression from occasional heartburn to serious respiratory complications often goes unrecognized until significant damage occurs.
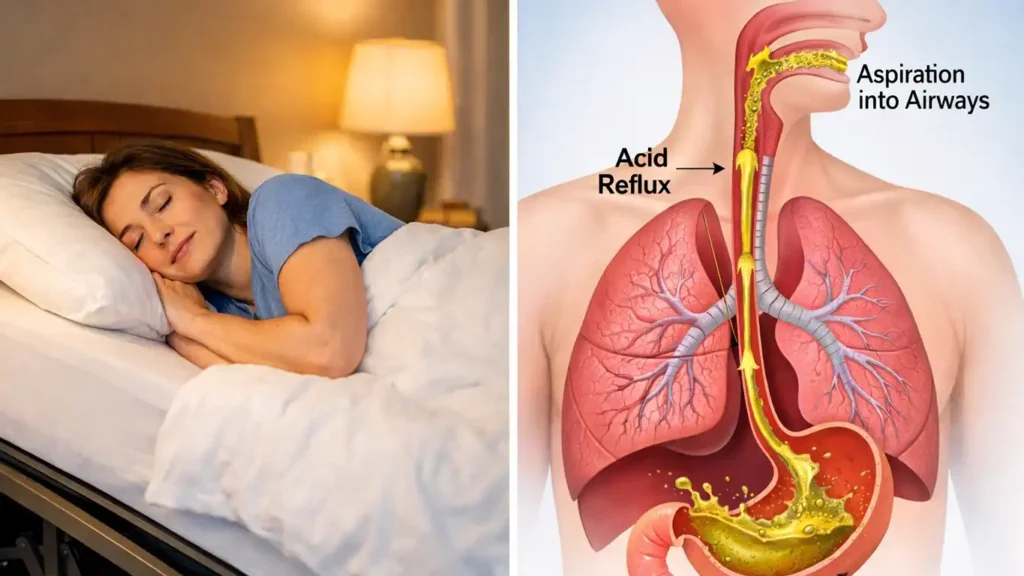
Today, I want to address a question that keeps many of my patients awake at night: can you die from acid reflux in your sleep? While death directly from acid reflux during sleep is rare, aspiration of stomach acid into the lungs can lead to severe pneumonia, respiratory failure, and in vulnerable populations, potentially fatal outcomes if left untreated.
By the end of this article, you’ll understand the mechanisms behind nocturnal GERD dangers, recognize emergency warning signs, and learn evidence-based strategies to protect yourself. Moreover, you’ll discover when lifestyle changes aren’t enough and why professional evaluation can literally save your life. Let’s normalize this conversation and empower you with the knowledge you need.
What Exactly Is GERD (Gastroesophageal Reflux Disease)?
The Basic Mechanism
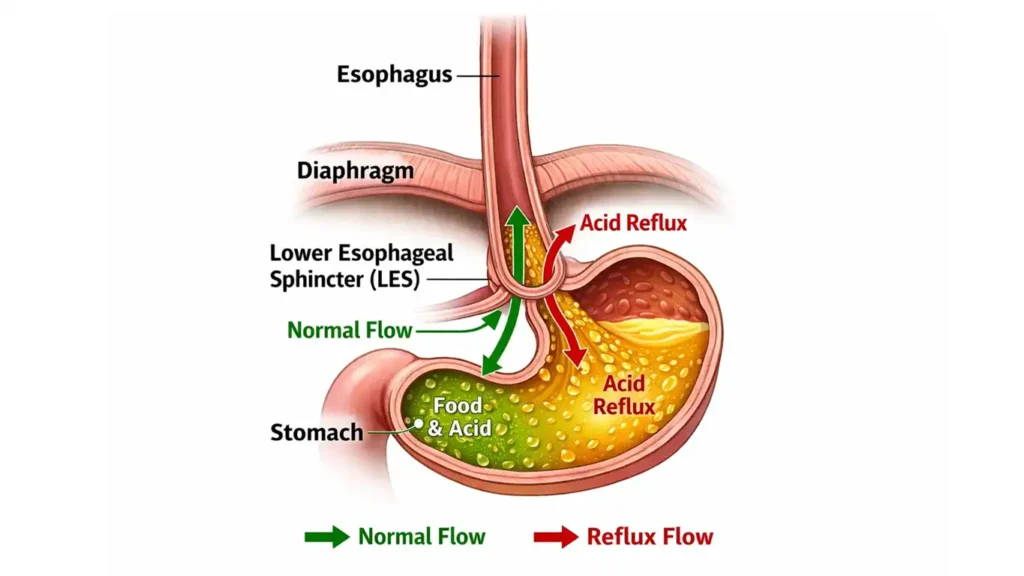
GERD occurs when stomach acid flows backward into your esophagus, the tube connecting your mouth to your stomach. Think of it like a drainage problem in your home. Normally, a muscular valve called the lower esophageal sphincter acts like a one-way door, allowing food down but keeping acid from coming back up.
However, when this valve weakens or relaxes inappropriately, acid escapes upward. Occasional heartburn happens to everyone. Chronic GERD means this backflow occurs regularly, causing persistent symptoms and potential tissue damage. The difference matters because while occasional reflux is annoying, chronic GERD can lead to fatal GERD complications over time.
The Anatomy Behind the Problem
Your body has multiple protective mechanisms working together. First, the gastroesophageal valve complex creates a tight seal. Second, your diaphragm muscle wraps around the esophagus where it passes from chest to abdomen, creating what doctors call a “pinchcock effect.” Third, the natural angle at which your esophagus enters your stomach provides additional protection.
When these mechanisms fail, either through anatomical abnormalities or functional problems, acid flows freely upward. Some people are born with weaker valves. Others develop problems from lifestyle factors, obesity, or hiatus hernias. Understanding why your body’s defenses have broken down helps guide the right treatment approach.
Why Does Acid Reflux Happen? Understanding the Root Causes
Anatomical Abnormalities
Certain structural problems predispose you to GERD. A hiatus hernia occurs when part of your stomach pushes through the diaphragm opening into your chest cavity. This disrupts the normal valve mechanism and makes reflux much more likely. Additionally, some people have naturally looser lower esophageal sphincters from birth.
Structural defects in the diaphragm muscle itself can also compromise protection. Natural variations in esophageal positioning may create angles that don’t effectively prevent backflow. These anatomical issues typically require more aggressive management because lifestyle changes alone won’t fix structural problems.
Functional Problems
Even with normal anatomy, functional issues can trigger reflux. Temporary valve weakness from certain foods, medications, or hormonal changes creates episodes of acid escape. Increased abdominal pressure from obesity, pregnancy, or tight clothing forces acid upward despite a functioning valve.
Furthermore, delayed stomach emptying means acid sits longer, increasing reflux risk. Lifestyle factors like smoking, alcohol, and certain medications relax the sphincter inappropriately. Identifying whether your GERD stems from anatomical or functional causes determines your treatment path.
Can You Die from Acid Reflux in Your Sleep? The Real Dangers
Understanding Aspiration Pneumonia Acid Reflux Connection
Here’s where nighttime acid reflux death becomes a genuine concern. When you’re asleep, your protective reflexes diminish. Normally, if acid reaches your throat while awake, you cough, clear your throat, or swallow it back down. During sleep, especially deep sleep, these protective mechanisms don’t work as efficiently.
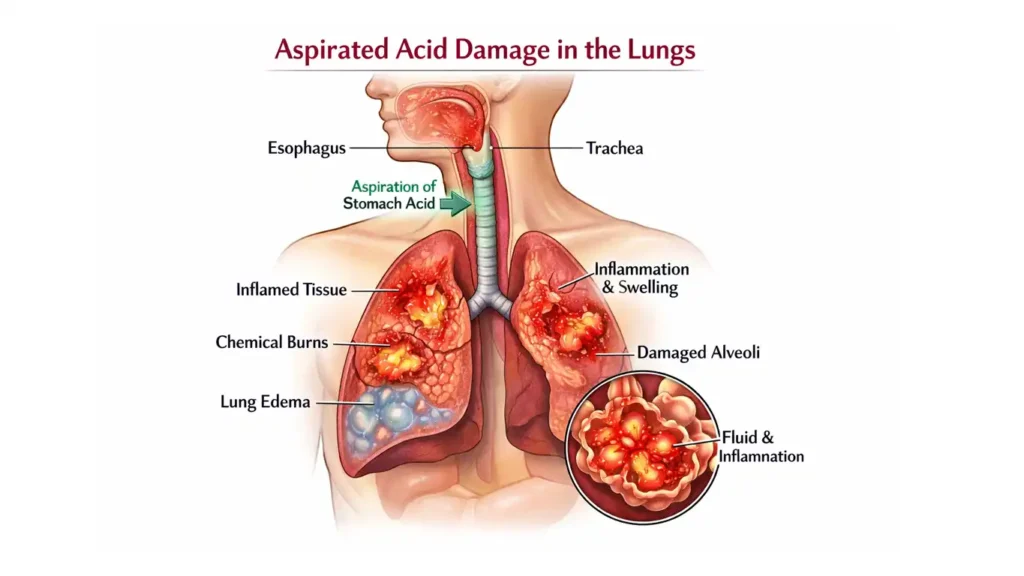
Consequently, acid can silently trickle into your airway and lungs, a process called aspiration. Your lungs aren’t designed to handle stomach acid. When acid enters lung tissue, it causes severe chemical burns, inflammation, and bacterial infection. This condition, aspiration pneumonia acid reflux, can rapidly progress to respiratory failure in vulnerable individuals.
Elderly patients, those with weakened immune systems, and people with neurological conditions face the highest risk. However, even healthy adults can develop serious complications from repeated nighttime aspiration. The acid doesn’t just irritate; it actively damages delicate lung tissue and creates an environment where dangerous bacteria thrive.
💡 Pro Tip: If you wake up choking, coughing, or gasping for air at night, don’t dismiss it as “just heartburn.” These are emergency warning signs that acid is entering your airway and require immediate medical evaluation.
Short-Term Complications That Escalate Risk
Beyond aspiration, nocturnal reflux creates multiple dangerous scenarios. Esophagitis, or inflammation of the food pipe, causes painful ulcers that can bleed. Severe bleeding can lead to anemia or, in extreme cases, life-threatening hemorrhage. Throat irritation triggers chronic cough, which many patients mistake for allergies or bronchitis.
Respiratory problems multiply when acid irritates your airways repeatedly. You might develop asthma-like symptoms, chronic bronchitis, or recurrent lung infections. Bad breath and altered taste sensations signal ongoing tissue damage. These symptoms impact your daily quality of life while simultaneously indicating progressive disease that needs intervention.
Long-Term Fatal GERD Complications
Over years of untreated reflux, Barrett’s esophagus develops in some patients. This precancerous condition occurs when chronic acid exposure causes your esophageal lining to transform into intestinal-type tissue. While Barrett’s esophagus itself isn’t immediately dangerous, it carries a significantly elevated risk of esophageal cancer from GERD.
Esophageal cancer remains one of the deadliest cancers, with five-year survival rates around 20 percent. Most patients receive diagnosis only after the disease has advanced significantly. Therefore, preventing Barrett’s esophagus through early GERD treatment literally prevents cancer deaths years down the line.
Chronic lung infections from repeated aspiration can cause permanent lung damage. Persistent bronchitis weakens respiratory function over time. Sleep disturbances from chronic cough and choking episodes create cascading health problems including cardiovascular disease, diabetes, and cognitive decline. The interconnections between untreated GERD and overall mortality become clear when you examine long-term outcomes.
The Danger of “Silent GERD”
Perhaps most frightening is silent GERD, where you experience minimal or no heartburn despite ongoing acid damage. I’ve seen patients who suffered years of throat clearing, chronic cough, and respiratory problems without realizing GERD was the culprit. Their esophageal tissue had become so damaged that nerve endings no longer registered pain from acid exposure.
These patients often have advanced disease by the time they receive proper diagnosis. Their risk of Barrett’s esophagus mortality and esophageal cancer climbs significantly. Silent GERD especially affects elderly patients, who may attribute symptoms to aging rather than treatable disease. Early detection becomes critical because you can’t rely on heartburn to warn you of danger.
Who Gets GERD? Risk Factors and Demographics
Age and Population Patterns
GERD most commonly affects middle-aged adults, but I’ve treated patients from teenagers to individuals in their nineties. The condition doesn’t discriminate by age, though risk factors accumulate over decades. Elderly patients face particular diagnostic challenges because their symptoms often masquerade as other conditions.
Moreover, older adults frequently see multiple specialists before receiving correct diagnosis. They visit primary care doctors for chronic cough, ENT specialists for throat problems, and pulmonologists for breathing difficulties. Meanwhile, the underlying GERD continues causing damage. Underdiagnosis in this population contributes to preventable complications and suffering.
The Misdiagnosis Journey
Have you been treated repeatedly for conditions that never fully resolve? This pattern suggests an underlying cause that hasn’t been identified. GERD symptoms mimic so many other problems that patients often undergo months or years of inappropriate treatment before someone considers reflux as the root cause.
I encourage my patients to think comprehensively about their symptoms. When you have multiple seemingly unrelated problems like chronic cough, hoarseness, dental erosion, and sleep disturbances, GERD might be the common thread connecting them all. Advocating for thorough evaluation can short-circuit the misdiagnosis journey and get you to effective treatment faster.
Recognizing the Warning Signs: GERD Symptoms
Classic Symptoms
Heartburn creates a burning sensation behind your breastbone, often worse after meals or when lying down. Regurgitation means tasting acid or partially digested food in the back of your throat. Difficulty swallowing suggests narrowing from chronic inflammation. Chest pain from GERD can frighten you into thinking you’re having a heart attack.
These classic symptoms make diagnosis straightforward when present. However, many patients experience atypical presentations that complicate recognition. Understanding the full spectrum of GERD symptoms empowers you to connect dots that might otherwise seem unrelated.
Atypical Symptoms Often Missed
Chronic nighttime cough represents one of the most common atypical presentations. The cough typically worsens when you lie down because gravity no longer helps keep acid in your stomach. Persistent sore throat, especially in the morning, signals overnight acid exposure. Hoarseness or voice changes occur when acid irritates your vocal cords.
Additionally, bad breath despite excellent oral hygiene suggests acid reflux. Dental erosion and discoloration happen because acid wears away tooth enamel. Disrupted sleep patterns affect every aspect of health, from mood to immune function. Respiratory issues without obvious cause should always trigger consideration of GERD as a potential culprit.
💡 Pro Tip: Keep a symptom diary tracking when symptoms occur, what you ate, your sleep position, and severity. Patterns emerge that help your doctor make accurate diagnosis and tailor treatment to your specific triggers.
GERD vs. Heart Attack: Critical Distinctions
This distinction can literally save your life. Chest pain from GERD typically feels like burning, occurs after eating, improves with antacids, and worsens when lying down. Heart attack pain often feels like pressure or squeezing, may radiate to your arm or jaw, doesn’t improve with antacids, and may come with shortness of breath, sweating, or nausea.
However, some heart attacks present atypically, especially in women and diabetics. Inferior wall heart attacks can cause upper abdominal pain mistaken for indigestion. Therefore, any new or severe chest pain warrants emergency evaluation with ECG and cardiac enzymes. Never assume chest pain is “just heartburn” without ruling out cardiac causes first.
When should you go to the ER? Severe chest pain, especially if accompanied by shortness of breath, arm pain, jaw pain, sweating, nausea, or lightheadedness, requires immediate emergency care. Better to have a false alarm than delay treatment for a heart attack.
Other Conditions That Can Cause Similar Symptoms
Peptic ulcers from H. pylori bacteria or NSAID use create burning upper abdominal pain. Pancreatitis, especially in people who consume alcohol heavily, causes severe epigastric pain. Lung infections can mimic the respiratory symptoms of GERD. Comprehensive evaluation rules out these alternative diagnoses before committing to long-term GERD treatment.
When Should You See a Doctor?
Red Flag Timeline
Symptoms lasting more than one to two weeks warrant medical evaluation. Don’t wait months hoping problems resolve spontaneously. If reflux interferes with daily activities, disrupts your sleep, or causes you to modify your lifestyle significantly, you need professional help.
Chronic nighttime cough deserves particular attention given the aspiration risks we discussed. Any symptoms that progressively worsen over time signal advancing disease that won’t improve without intervention. Early evaluation prevents complications and improves treatment outcomes.
Urgent Warning Signs That Demand Immediate Care
Certain GERD emergency symptoms require urgent or emergency evaluation. Severe chest pain needs cardiac workup first, always. Difficulty swallowing or painful swallowing suggests significant esophageal inflammation, stricture, or potentially cancer. Unintended weight loss raises serious concern for malignancy.
Vomiting blood or passing dark, tarry stools indicates gastrointestinal bleeding requiring emergency care. Symptoms in patients over 50 carry higher cancer risk and warrant expedited endoscopy. Choking on acid reflux while sleeping, especially if it happens repeatedly, signals dangerous aspiration risk requiring immediate intervention.
Risk Factors That Make GERD Worse
Obesity and Body Weight
Excess weight increases abdominal pressure, forcing acid upward even with a functioning valve. The mechanics are simple: more pressure in your abdomen means more force pushing stomach contents toward your esophagus. Furthermore, people carrying extra weight often consume larger meal portions, overdistending the stomach and weakening the lower esophageal sphincter over time.
Weight management represents one of the most effective GERD treatments available. Even modest weight loss of 10 to 15 pounds can dramatically reduce symptoms in overweight patients. I’ve seen patients completely eliminate their need for medications simply by achieving healthier body weight through sustainable lifestyle changes.
Pregnancy
Pregnancy creates temporary increased abdominal pressure as the growing uterus pushes upward. Hormonal changes during pregnancy also relax the lower esophageal sphincter. Consequently, many pregnant women experience reflux for the first time or notice worsening of pre-existing GERD.
Fortunately, pregnancy-related reflux typically resolves after delivery once abdominal pressure normalizes and hormones return to baseline. Management during pregnancy focuses on safe lifestyle modifications and, when necessary, medications considered safe for developing babies.
Medications That Trigger GERD
Many common medications worsen reflux by either irritating stomach lining or relaxing the lower esophageal sphincter. Aspirin and NSAIDs like ibuprofen directly damage the stomach and esophageal lining. Blood pressure medications, particularly calcium channel blockers, relax smooth muscle including the sphincter.
Oral contraceptive pills affect hormone levels that can influence sphincter tone. Chemotherapy drugs cause severe gastrointestinal irritation. Therefore, doctors often prescribe PPIs (proton pump inhibitors) alongside these medications to protect your digestive tract. H. pylori treatment itself requires long-term acid suppression. Even antibiotics for unrelated infections can trigger reflux by irritating your stomach.
Never stop prescribed medications without consulting your doctor, but do discuss GERD symptoms so protective strategies can be implemented. Sometimes, alternative medications without reflux side effects can be substituted.
Lifestyle and Dietary Triggers
Foods and Beverages to Avoid
Spicy foods directly irritate your esophageal lining and increase acid production. Deep-fried and high-fat foods delay stomach emptying, keeping acid present longer and increasing reflux likelihood. Alcohol relaxes the lower esophageal sphincter while simultaneously increasing acid production, a double threat.
Excessive coffee and tea, particularly more than one to two cups daily, also relax the sphincter. Chocolate, peppermint, carbonated beverages, citrus fruits, and tomato-based products represent other common triggers. However, trigger foods vary individually, so identifying your personal culprits through systematic elimination helps tailor dietary management.
Eating Habits That Help
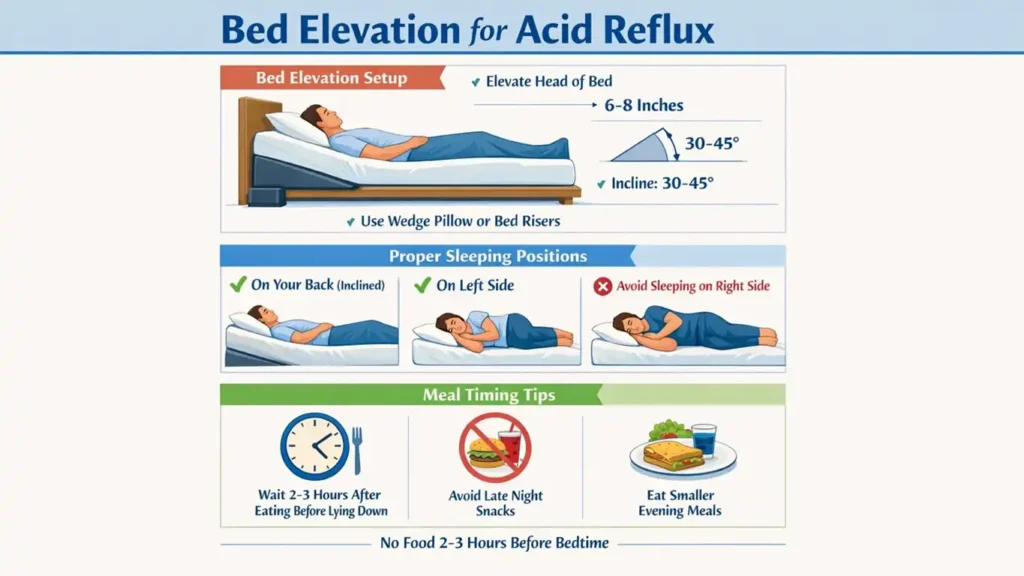
How you eat matters as much as what you eat. Smaller, more frequent meals prevent stomach overdistension. Large meals stretch your stomach, weaken the valve, and increase reflux risk significantly. Avoid lying down for at least three hours after eating. Gravity helps keep acid down, so maintaining upright posture after meals provides natural protection.
Elevating the head of your bed six to eight inches using blocks under the bed frame (not just pillows) prevents nighttime reflux treatment. Don’t eat within three hours of bedtime, allowing your stomach to empty before you lie down. These simple sleeping position acid reflux modifications can dramatically reduce nighttime symptoms and aspiration risk.
The Role of Stress
The brain-gut axis represents a bidirectional communication highway between your nervous system and digestive tract. Stress triggers hormone release that increases stomach acid production. Moreover, stress alters gut motility and may affect sphincter function. Chronic stress compounds GERD symptoms through multiple pathways.
Therefore, stress management isn’t just about feeling better emotionally; it’s a legitimate medical intervention for GERD. Meditation, regular exercise, adequate sleep, therapy, and other stress reduction techniques can measurably improve reflux symptoms and reduce your need for medications.
Diagnosing GERD: From Symptoms to Confirmation
Initial Clinical Assessment
Your doctor begins with a detailed symptom history. When do symptoms occur? What makes them better or worse? How long have you experienced them? What treatments have you tried? A thorough physical examination looks for complications like dental erosion, throat inflammation, or respiratory problems.
For recent-onset symptoms lasting just a few days, a trial of lifestyle modifications and short-term medication may suffice. Many patients respond well to initial treatment without needing invasive testing. However, persistence despite appropriate treatment signals the need for further investigation.
When Further Testing Is Needed
Failure to respond to appropriate medication raises concern about alternative diagnoses or severe GERD. Symptom duration matters: the longer you’ve had reflux, the higher your risk of complications requiring investigation. Age considerations are critical, especially if you’re over 50, because cancer risk increases substantially with age.
Upper GI Endoscopy: The Gold Standard
Endoscopy involves passing a thin, flexible camera through your mouth while you’re under mild sedation. The gastroenterologist examines your esophagus, the valve, your stomach, and the first part of your small intestine. This procedure provides invaluable information about valve laxity, hiatus hernia presence, stomach ulcers, esophageal strictures, and can detect cancer.
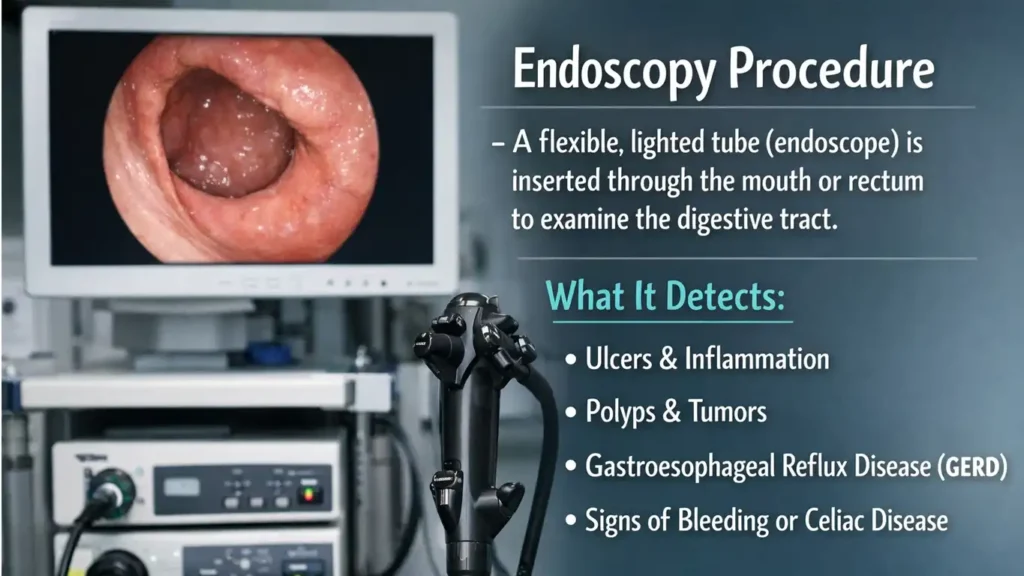
Is endoscopy painful? Most patients tolerate it well under conscious sedation, experiencing minimal discomfort and no memory of the procedure. The brief test provides diagnostic clarity that guides definitive treatment. I recommend endoscopy for anyone over 50 with chronic GERD symptoms and anyone with alarm symptoms regardless of age.
Tissue Sampling During Endoscopy
During endoscopy, your doctor takes small tissue samples for analysis. Biopsies test for H. pylori bacteria that may require specific antibiotic treatment. Samples from suspicious areas rule out malignancy. Importantly, biopsies can identify Barrett’s esophagus, allowing early intervention before cancer develops.
Understanding GERD Severity
Indicators of Serious GERD
High-volume reflux where food comes up, not just acid, indicates severe disease. Barrett’s esophagus on endoscopy represents a precancerous condition requiring intensive monitoring and treatment. Respiratory complications like pneumonia, bronchitis, or recurrent lung infections signal dangerous aspiration.
Throat inflammation, dental damage, and persistent bad taste indicate ongoing tissue injury. Comprehensive evaluation considers all related symptoms, not just heartburn. The pattern of complications guides treatment intensity and urgency.
Treatment Options: From Lifestyle to Surgery
Can GERD Go Away on Its Own?
Temporary episodes from overeating, alcohol, or rich meals often resolve without intervention once the triggering event passes. Lifestyle modifications can effectively control functional GERD where anatomy remains normal. However, anatomical problems like loose valves, hiatus hernias, or diaphragm defects persist without surgical correction.
Therefore, some patients need ongoing management. Understanding whether your GERD stems from temporary triggers versus structural problems helps set realistic expectations about treatment duration and approach.
Lifestyle Modifications That Actually Work
Weight management through sustainable diet and exercise reduces abdominal pressure. Dietary changes focusing on smaller meals and avoiding trigger foods provide measurable benefit. Posture strategies and meal timing prevent gravitational reflux. Head elevation during sleep represents one of the most effective nighttime reflux treatment approaches.
Stress reduction through meditation, therapy, or other techniques addresses the brain-gut axis. Smoking cessation improves sphincter function and reduces cancer risk. These interventions work synergistically: combining multiple lifestyle changes produces better results than any single intervention alone.
💡 Pro Tip: Start with three achievable changes rather than trying to overhaul everything at once. Master those, then add more. Sustainable change beats short-term perfection that you can’t maintain long-term.
Medical Management of GERD
Antacids: What They Do and Don’t Do
Antacids work by neutralizing existing stomach acid or reducing acid production. They provide temporary symptom relief but don’t cure GERD. The underlying valve problem or anatomical abnormality remains unchanged. Over-the-counter solutions have limitations and shouldn’t substitute for professional evaluation when symptoms persist.
The Danger of Self-Medication
Self-medication leads to wrong dosages, inappropriate drugs for your specific condition, and delayed diagnosis of serious underlying problems. What works for your friend may not work for you. Professional guidance ensures you receive appropriate treatment at the right dose for adequate duration while monitoring for complications.
Proton Pump Inhibitors (PPIs) and Prescription Treatment
PPIs reduce stomach acid production by blocking the cellular pumps that generate acid. Appropriate initial duration typically runs two to four weeks. H. pylori treatment requires two weeks of antibiotics plus six additional weeks of PPIs. Your doctor determines when to continue versus when to stop based on symptom response and endoscopy findings.
Limitations of Long-Term Medication
Medications don’t provide 24-hour protection, leaving windows when acid can still reflux. Over time, tolerance develops where the same dose becomes less effective. Prolonged PPI use carries side effects including increased infection risk, bone fracture risk, and potential nutrient malabsorption.
Generally, I don’t recommend PPIs beyond two to three months without reevaluation. When patients require longer treatment, surgery often becomes the better option, offering potential cure without ongoing medication side effects. This conversation represents an important decision point in GERD management.
Special Considerations for Elderly Patients
Elderly patients may not tolerate surgery well due to other health conditions. For them, balancing risks and benefits of long-term medication versus surgical risk requires individualized assessment. Quality of life considerations help guide decisions when neither option is ideal.
When Surgery Becomes Necessary
Candidates for Surgical Intervention
Surgery is considered for patients who fail medical management or whose symptoms return after stopping medications. Presence of hiatus hernia often requires surgical repair. Very lax sphincters don’t respond adequately to medications. Barrett’s esophagus may warrant surgery to prevent cancer progression.
Respiratory complications from aspiration, chronic throat infections, and other extra-esophageal manifestations that don’t improve with medication may benefit from surgical intervention. However, patient selection remains critical: typically, only two out of every ten patients I evaluate actually need surgery. Careful selection ensures optimal outcomes.
Laparoscopic Fundoplication: The Standard Surgical Approach
This minimally invasive keyhole technique involves several steps. First, the surgeon tightens the diaphragm opening where the esophagus passes through. Second, the esophagus is brought four to five centimeters down into the abdomen. Third, the upper part of the stomach is wrapped around the esophagus, creating a new valve mechanism.
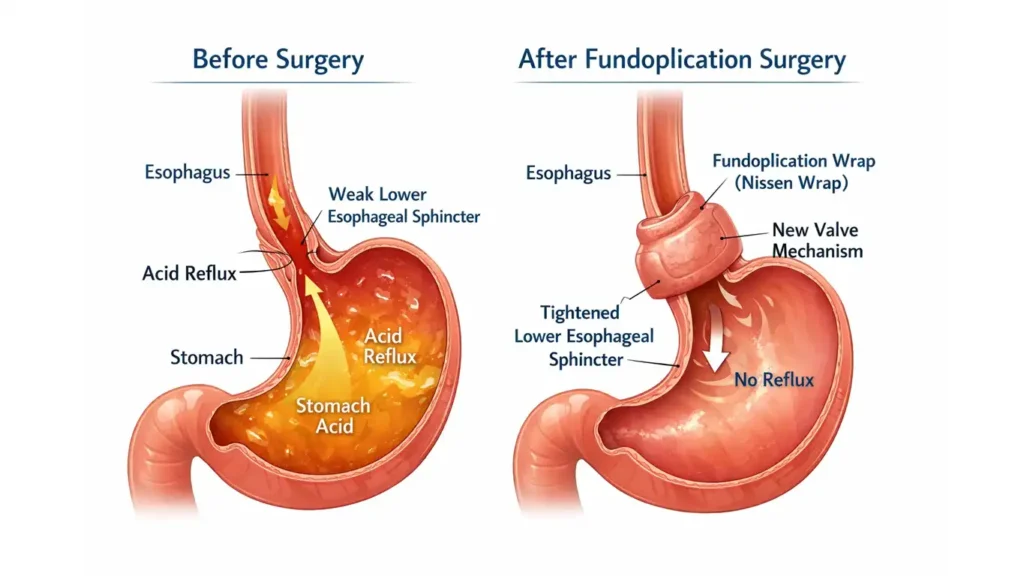
This wrap prevents acid from escaping upward while still allowing food to pass downward. Most patients receive a complete 360-degree wrap. Elderly patients with poor esophageal muscle tone may receive a partial posterior wrap, allowing easier food passage while still preventing reflux.
Newer Experimental Options
Endoscopic fundoplication techniques performed through the mouth without external incisions are being investigated. However, these lack long-term data and standardized results. They remain in the investigative phase and aren’t yet recommended as standard treatment. Traditional laparoscopic surgery remains the gold standard with proven outcomes.
Surgery Outcomes and Considerations
Success Rates and Permanence
Surgery offers the chance for permanent cure in appropriately selected patients. Critical patient selection ensures optimal results. When the right patient undergoes the right procedure by an experienced surgeon, outcomes are excellent with high satisfaction rates.
Surgical Risks
Standard anesthesia risks apply as with any surgery. Bleeding during the procedure is possible but manageable. Wound infection remains rare with proper technique. Complications are addressed immediately during surgery. Overall, the safety profile of laparoscopic fundoplication is excellent when performed by experienced surgeons.
Can GERD Return After Surgery?
Recurrence after properly performed surgery in appropriately selected patients is very rare. Patients who receive partial wraps may experience minimal reflux but with much better control than before surgery. Complete cure may not be achievable in all cases, especially elderly patients with compromised esophageal function. However, even partial improvement significantly enhances quality of life.
Common GERD Myths: True or False
| Myth | Truth | Explanation |
|---|---|---|
| Coffee and tea increase acid reflux risk | TRUE | Excessive consumption relaxes the valve; moderation is key |
| Untreated GERD can cause cancer | TRUE | Long-term progression: GERD → Barrett’s → esophageal cancer |
| Children cannot have GERD | FALSE | Less common but definitely occurs; youngest surgery patient was 14 |
| Stress causes acid reflux | PARTIALLY TRUE | Stress increases acid production through brain-gut axis |
| Spicy foods should always be avoided | TRUE | Spicy foods increase reflux episodes significantly |
| Lifelong medication is needed if surgery isn’t an option | FALSE | No patient should be on GERD medication indefinitely |
| GERD doesn’t affect sleep | FALSE | Significantly disrupts sleep; common patient complaint |
Preventing GERD Deaths: Your Action Plan
Immediate Steps You Can Take
Elevate your bed head six to eight inches tonight. Stop eating three hours before bedtime starting now. Identify and eliminate your top three dietary triggers this week. Schedule that doctor’s appointment you’ve been postponing if symptoms have lasted more than two weeks.
Long-Term Strategies
Work toward healthy body weight through sustainable changes. Manage stress through proven techniques that fit your lifestyle. Follow treatment plans consistently and report medication failures promptly. Get recommended screening endoscopy if you’re over 50 with chronic symptoms.
When to Seek Emergency Care
Go to the ER immediately for severe chest pain, difficulty breathing, vomiting blood, or choking episodes that don’t resolve quickly. Don’t gamble with symptoms that could indicate life-threatening complications. Emergency evaluation can save your life.
Key Takeaways: Don’t Ignore the Warning Signs
GERD Is More Common Than You Think
This widespread condition affects all age groups but often goes undiagnosed or misdiagnosed. The symptoms extend far beyond heartburn to include chronic cough, chest pain, respiratory problems, sleep disturbances, and dental issues.
Serious Complications Cannot Be Ignored
Esophageal damage, Barrett’s esophagus, cancer risk, and lung complications represent real dangers of untreated GERD. Early action prevents these outcomes and preserves your health and quality of life.
The Importance of Early Action
Don’t dismiss persistent heartburn as “just acidity.” Underlying serious problems may be developing that need investigation. Proper diagnosis and treatment prevent complications while significantly improving how you feel day-to-day.
Conclusion: Taking Control of Your Health
Understanding GERD empowers you to recognize symptoms early and seek appropriate care. Multiple effective treatment options exist, from lifestyle modifications for mild cases to medical management and surgical solutions for severe disease. Personalized treatment based on your individual needs offers the best outcomes.
Can you die from acid reflux in your sleep? While rare, aspiration pneumonia and other fatal complications can occur, particularly in vulnerable populations. However, with proper recognition, diagnosis, and treatment, these tragic outcomes are preventable. Don’t ignore persistent heartburn or atypical symptoms. Consult your healthcare provider if symptoms last beyond one to two weeks.
Modern medicine offers excellent solutions for GERD. Early intervention prevents serious long-term complications. Better quality of life is not just possible but probable when you take action. Your health matters, and normalizing these conversations helps everyone receive the care they deserve. Take that first step today.

 By
By
 By
By



 By
By






