
If you have ever typed is there a girl version of erectile dysfunction into a search bar, you are not alone. You are also not being dramatic. This topic matters now because stress is high, relationships are busy, and many people still feel embarrassed asking for help. So they suffer in silence. I want you to know this is common, it is real, and it is often treatable.
If you want to hear the source discussion that shaped this approach, you can watch the first video on female sexual dysfunction basics and the second video on evaluation and treatment pathways.

Female sexual dysfunction: what it is, why it happens, and how to get help
I am Dr. Muhammad Usman Arif. I am fellowship-trained and I spend my days in men’s sexual health. But I also care deeply about the couple, because sexual health rarely lives in one body. When one partner struggles, the relationship often feels it.
In simple terms, female sexual dysfunction means problems that reduce desire, pleasure, enthusiasm, or comfort in sexual relationships. It can look like low libido in women, female arousal disorder, difficulty reaching orgasm, or pain.
Here is what I will walk you through, step by step:
- The four main categories.
- The emotional and relationship impact.
- What a women’s sexual health evaluation often includes.
- A treatment pathway that is practical and personal.
This is for individuals, couples, and anyone who feels stuck and unsure where to start.
What counts as a sexual dysfunction (and when it becomes a real problem)
A practical definition is this: if something takes away your desire, pleasure, or enthusiasm for sexual connection, it counts. The key detail is impact. Does it affect your mood, confidence, relationship, or quality of life?
You might say:
- “I love my partner, but my body is not cooperating.”
- “I avoid sex because it hurts.”
- “I want to want it, but the spark is gone.”
So here is the real question: are you distressed by it, or is it simply a phase you feel okay about? If it is causing stress, shame, or conflict, then it deserves attention. And yes, you deserve care that takes this seriously.
The 4 categories of female sexual dysfunction
People often compare this to male erectile dysfunction, but the “match” is not one-to-one. A clearer way is to map common patterns side by side.
| Common concern | Often seen in men | Often seen in women |
|---|---|---|
| Desire | Low desire | Low desire with distress |
| Arousal response | Erection problems | Arousal response problems, including vaginal dryness and arousal mismatch |
| Orgasm | Trouble reaching orgasm | difficulty reaching orgasm |
| Pain | Pain can occur | sexual pain disorders in women and other painful sex causes |
So, what should you watch for in your own life?
Low sexual desire (HSDD)
Low desire becomes a clinical concern when there is little or no interest in sex and you feel distress about it. One medical label you may hear is hypoactive sexual desire disorder HSDD. That label can feel heavy, but it also helps many people feel less alone.
Ask yourself:
- Do you miss wanting sex?
- Do you feel worry, guilt, or pressure because of it?
Those feelings matter, because they often drive anxiety, avoidance, and conflict.
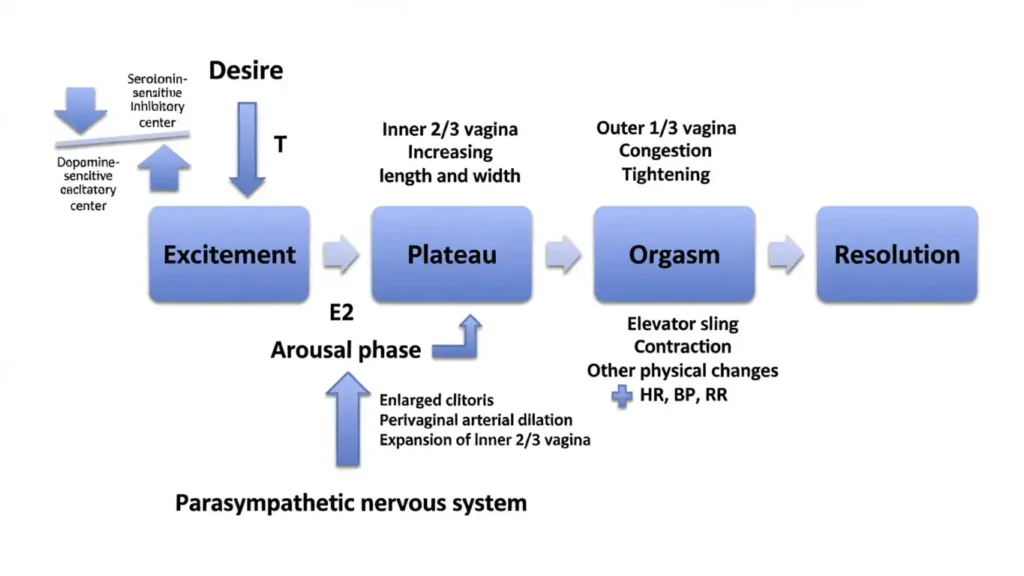
Sexual arousal disorder (is there a girl version of erectile dysfunction)
This is about the body not responding the way you expect during sexual activity. Mentally, you might feel connected, yet physically you feel flat. Many people describe it as “my mind is there, but my body is not.”
This is also where late-night searches like “trouble getting aroused female” come from. So if that is you, here is the important part: this is not a character flaw.
And because arousal is linked to comfort, vaginal dryness and arousal often show up together.
Orgasmic disorder
This can mean you cannot orgasm, or it is consistently hard to reach orgasm. Difficulty reaching orgasm can affect confidence fast, especially if you start thinking you are “broken.” You are not.
A useful question is: has it always been this way, or is it a change? Changes often point to a fixable driver, so that detail is worth sharing with your clinician.
Sexual pain disorders
Pain during sex or genital touch is never something you should push through. There are many painful sex causes, and the broader bucket is often called sexual pain disorders in women.
If you feel burning, sharp pain, or deep aching, pause and get evaluated. Pain is a signal, not a test of willpower.
Why low libido can hit so hard emotionally
Low desire is not just a bedroom issue. It can feel like an identity issue. I have heard people say they feel inadequate as a partner, or even “less of a woman.” That pain is real.
Desire can be influenced by both psychological and biological factors. So, it is not “all in your head,” and it is not “just hormones” either. It is usually a mix.
Let me ask you something gently: when did you start blaming yourself? And what would change if you treated this like a health concern instead of a personal failure?
Sometimes, the first healing step is naming it and realizing you are not the only one.
The relationship spiral: avoidance, assumptions, and disconnection
When sex becomes stressful, people avoid it. Avoidance is understandable, but it often backfires.

Here is the common spiral:
- One partner pulls back to avoid discomfort or shame.
- The other partner assumes it is rejection.
- Both partners stop talking.
- Resentment grows, and closeness fades.
Have you noticed how silence fills in the blanks with worst-case stories?
This is why communication matters. Even one sentence can change the direction: “This is hard to talk about, but I want us to be a team.”
Talk to your partner: how to turn it into a team problem (not a blame problem)
If you are wondering about how to talk to your partner about low libido, start simple and kind. You are not presenting a verdict. You are sharing a problem you want to solve together.
Try:
- “I care about us, and I want to understand what’s going on.”
- “I’m feeling stressed about sex, but I don’t want distance between us.”
- “Can we get help as a team?”
Pro Tip 🗣️: Use “I feel” plus “I want,” then ask for teamwork, not permission.
Team behaviors that help:
- Attend appointments together, if the patient wants that support.
- Agree on low-pressure intimacy while you seek care.
- Keep affection present, even if sex is paused.
Ask yourself: what would it feel like if this became a shared plan instead of a private burden?
Speak up: your sexual health concerns deserve real medical attention (is there a girl version of erectile dysfunction)
I want to be clear: sexual health is part of health. You have the right to bring it up. It is also the responsibility of clinicians to address it seriously.
So speak up. If you feel dismissed, you can seek a different clinician. That is not “doctor shopping.” That is self-respect.
What to prepare before your visit:
- Your top two symptoms, in plain words.
- When it started, and whether it is getting worse.
- How it affects your relationship and mood.
- A list of medications and major lifestyle changes.
Pro Tip 📝: Bring a short symptom log and your med list, it saves time and boosts clarity.
Why many women don’t know where to go (and why specialized clinics matter)
Many women do not know where to go for sexual concerns. And yes, some general clinics do not prioritize these issues. That can leave you feeling awkward, brushed off, or stuck.
Specialized clinics exist because sexual function is complex. It can involve tissues, hormones, nerves, muscles, emotions, and relationship dynamics. So a focused clinic is more likely to evaluate the full picture and offer a structured pathway.
If your first try was not helpful, do not let that be the final chapter. You deserve a clinician who listens.
What to expect at a visit: intake, questionnaires, and a thorough evaluation
A good visit is usually structured. You may fill out questionnaires first. Then you will have a detailed history and a physical exam that is guided by comfort and consent.
A solid women’s sexual health evaluation often looks at:
- Desire, arousal, orgasm, and pain patterns.
- Relationship context and stress load.
- Medical history, medications, and lifestyle.
You can ask:
- “What category do you think this fits?”
- “What factors are you considering?”
- “What are my options, and what is realistic?”
Good care feels organized, not rushed.
Identifying contributing factors: lifestyle, medications, and health history
Lifestyle factors can matter. Sleep, stress, and relationship tension can all shape desire and arousal. Medications can also play a role, so it is worth reviewing them.
Bring:
- Your full medication list.
- Any major life changes, like grief, new work stress, or postpartum shifts.
- A quick summary of what you have already tried.
The goal is not to blame your lifestyle. The goal is to find what is correctable.
Physical exam focus: pain, tissue changes, and comfort
A complete exam may feel similar to a gynecology visit. The clinician may look for physical drivers of pain and reduced pleasure, such as scar tissue or thinning of the vaginal wall.
This matters because tissue health can influence comfort and arousal. If sex hurts, the body learns to guard. That guarding can make future intimacy harder.
You can always say:
- “Please go slowly.”
- “I want to pause.”
- “Can you explain what you’re checking for?”
Consent and comfort are part of the treatment.
Lab work and hormones: what gets checked
Labs may include hormones like estrogen, progesterone, and testosterone. This is where topics like hormones and low libido often come up. Some people also ask about testosterone and female desire. The key is that testing helps identify patterns that might be treatable.

Still, labs are only one piece. Numbers do not replace your lived experience. So the best plans combine symptoms, exam findings, and labs.
If a hormonal problem is found, it can often be addressed. But outcomes vary, and it should be personalized.
The treatment “pathway”: building a roadmap that fits the person
A smart clinic often uses a pathway approach. It shows options upfront, then helps you choose a roadmap based on your goals, values, and medical findings. This reduces guesswork and shame.
Introducing a structured plan
A good plan feels like:
- Clear options.
- Shared decision-making.
- A timeline you can understand.
Ask: “What is step one, and what are we watching for?” Clarity lowers anxiety, and anxiety often worsens symptoms.
Therapy and counseling support: individual and couple-focused
Sex is physical, but it is also emotional and relational. Sexual therapists can help uncover barriers and reduce pressure. Sex therapy for couples can be especially helpful when miscommunication and resentment have built up.
This is not about blaming a partner. It is about rebuilding safety and teamwork, so the body can respond again.
Medical options for low desire
For some low desire disorders, there may be specialized medication options. I will not name drugs here because candidacy is personal and should be discussed with a clinician who knows your history.
The key message is hope with honesty: options exist, but not every option fits every person.
Treating sexual pain: comprehensive options described
Pain often needs a layered approach, because drivers can overlap.
Topical treatments
Clinics may use hormonal creams or compounded creams to support comfort. These are local options that may be considered when tissue health appears to be part of the problem.
Physical therapy support
Some patients benefit from pelvic floor physical therapy for sex pain, especially when muscle tension or nerve irritation is involved. This can be a game-changer for comfort, but it takes time and trust.
Pro Tip 🌿: If sex hurts, pause and shift to comfort-first care, not “push through” power.
Vaginal treatments mentioned (is there a girl version of erectile dysfunction)
Some clinics offer vaginal laser treatments such as Monalisa Touch, and radiofrequency treatments such as Therm IVA. These are discussed as ways to support vaginal wall health and comfort with intercourse.
Ask before choosing:
- “Am I a good candidate?”
- “What outcomes are realistic for me?”
- “What are alternatives?”
Addressing hormonal disorders as part of the plan
If a hormonal disorder is present, correcting it can be part of the roadmap. But it should be tied to symptoms, not just lab values. The best plans keep returning to one core goal: improving comfort, confidence, and connection in real life.
Privacy, discretion, and feeling safe getting care
Many people delay care because they fear embarrassment. So let me say this plainly: sexual concerns are medical concerns. Treatment can be discreet and private. A good clinic protects your dignity.
You also get to set boundaries:
- You can request a clinician you feel comfortable with.
- You can bring a partner or come alone.
- You can switch clinicians if you feel dismissed.
You deserve respect at every step.
Practical next steps for readers
Progress usually starts with small, clear moves.
A simple self-check: what category sounds most like you?
Which sounds closest?
- Low desire with distress.
- Arousal mismatch, including dryness or lack of response.
- Trouble reaching orgasm.
- Pain with sex or touch.
Write down:
- When it happens.
- What makes it better or worse.
- How it affects your emotions and relationship.
How to start the conversation with your partner
Use teamwork language:
- “I want closeness, and I want help.”
- “This is not about you being unattractive.”
- “Can we work on this together?”
Then ask a direct question: “What support would help me feel safe while we figure this out?”
How to advocate for yourself in healthcare
If you are wondering when to see a doctor for sexual problems, here are clear signs:
- Symptoms last for months and cause distress.
- Sex is painful.
- You are avoiding intimacy out of fear.
- Relationship tension is rising because of the issue.
You can also say: “I need a plan, not a shrug.” That is a fair request.
Closing: the main takeaways to reinforce
Female sexual concerns are common, real, and worth treating. The four categories help you name what is happening. Silence often creates distance, but clear talk can rebuild teamwork. Good care is structured, private, and personal.
Most importantly, you do not have to carry this alone. There are pathways forward, and there is room for hope, even if you feel stuck today.

 By
By
 By
By



 By
By







